

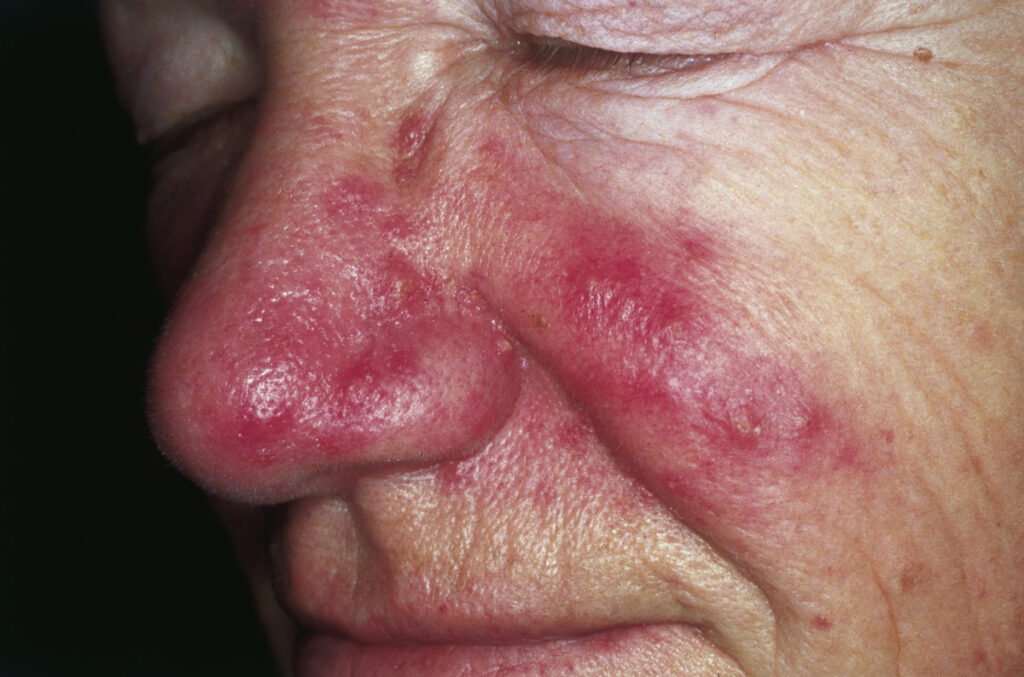
“My cheeks have been red for years. My family says it’s just my complexion. My beautician called it sensitive skin and sold me calming creams. One doctor said it was acne. Another said eczema. Nobody could tell me why my face burns after every meal, why spicy food makes me flush instantly, or why my nose is getting progressively larger and redder.”
Namita, a 38-year-old teacher from Delhi, had been living with undiagnosed rosacea for nearly a decade.
By the time she reached my clinic, her condition had progressed from simple flushing to persistent redness, visible blood vessels, and rhinophyma- thickening of the nose tissue that could have been prevented entirely with early intervention.
Her story isn’t unusual. Rosacea is one of the most consistently misdiagnosed conditions in Indian dermatology, and the reasons are understandable.
In lighter Caucasian skin, rosacea’s classic redness is immediately obvious.
In Indian skin, medium to dark brown tones with higher melanin – that same redness appears as subtle darkening, uneven patches, or what looks like stubborn pigmentation. Add cultural assumptions that “Indians don’t get rosacea” (fundamentally wrong), and you have thousands of patients suffering unnecessarily.
As a dermatologist practicing in Delhi, I estimate that for every rosacea patient I diagnose, at least three others are sitting at home applying the wrong treatments, worsening their condition, and wondering why their face never seems to calm down.
This guide provides everything you need to know about rosacea in Indian skin – what it actually looks like on darker complexions, why our environment worsens it, what treatments work, and, critically, what to avoid.
What Exactly Is Rosacea गुलाब रोग ?
Rosacea is a chronic inflammatory skin condition primarily affecting the central facecheeks, nose, chin, forehead, and around the eyes. It involves abnormal blood vessel reactivity, immune system dysfunction, and often colonization by specific microorganisms.
Key characteristics:
- Chronic, recurring condition (not curable but manageable)
- Primarily affects central facial areas
- Involves both vascular and inflammatory components
- Progressive without treatment
- Multiple subtypes with different presentations
- Triggers vary by individual
What rosacea is NOT:
- Simple sunburn
- Acne (though often confused)
- Allergic reaction
- Normal skin flushing
- Poor hygiene
- Alcohol-related (though alcohol worsens it)
Why Indian Patients Get Misdiagnosed
Rosacea गुलाब रोग in Indian skin looks different:
In Caucasian skin: Obvious bright red flushing, visible instantly against pale background
In Indian skin:
- Subtle deepening of natural skin tone
- Brownish-red or dusky discoloration
- Appears as “uneven skin tone” rather than classic redness
- Post-inflammatory darkening masks underlying inflammation
- Persistent “tired looking” appearance
- Often dismissed as pigmentation issue
Common misdiagnoses:
- Acne vulgaris
- Eczema or dermatitis
- Perioral dermatitis
- Seborrheic dermatitis
- Simple hyperpigmentation
- “Sensitive skin”
- Melasma
The confusion with acne: Rosacea can cause acne-like bumps (papules and pustules), leading to months of acne treatment that makes rosacea worse. Standard acne treatments benzoyl peroxide, salicylic acid, harsh cleansers – significantly irritate rosacea.
For understanding the difference between conditions causing facial breakouts, our acne treatment guide provides helpful diagnostic context.
Types of Rosacea: Which Do You Have?
Understanding your rosacea subtype is essential because treatment differs significantly between types.
Type 1: Erythematotelangiectatic Rosacea (ETR)
Primary features:
- Flushing and persistent central facial redness
- Visible blood vessels (telangiectasias)
- Burning or stinging sensations
- Skin feels rough or scaly
- Swelling may occur
How it looks in Indian skin:
- Persistent dusky or brownish-red central face discoloration
- Visible small blood vessels (often mistaken for aging changes)
- Skin appearing “permanently irritated”
- Frequent complaints of skin “burning” without obvious cause
Triggers particularly problematic:
- Temperature extremes (very relevant in Delhi – extreme cold to heated indoors)
- Hot beverages
- Exercise
- Spicy foods
- Alcohol
Treatment focus: reducing flushing, strengthening vessels, avoiding triggers
Type 2: Papulopustular Rosacea
Primary features:
- Acne-like breakouts in central face
- Papules (red bumps) and pustules (pus-filled bumps)
- Persistent background redness
- No comedones (blackheads/whiteheads—key difference from acne)
How it looks in Indian skin:
- Inflammatory bumps on cheeks and nose
- Background darkening easily confused with post-acne marks
- Often treated for years as acne without improvement
- Breakouts don’t respond to standard acne treatments
Critical distinction from acne:
- No blackheads or whiteheads in rosacea
- Central face distribution (forehead, temples less affected)
- Background redness/flushing present
- Worsens with standard acne treatments
- Different age of onset (usually 30s-50s)
Treatment focus: Anti-inflammatory approach, specialized medications, gentle skincare
Type 3: Phymatous Rosacea
Primary features:
- Skin thickening and irregular surface
- Most commonly affects nose (rhinophyma)
- Can affect chin, cheeks, forehead, ears
- Enlarged pores
- Nodular, bumpy texture
In Indian skin:
- Thickening may appear darker than surrounding skin
- Nose enlargement gradual and often dismissed as “aging”
- More common in men
- Usually develops from untreated Type 1 or 2
Important: This is preventable with early treatment of other rosacea types. Advanced rhinophyma requires surgical intervention.
Treatment focus: Medical management to prevent progression, surgical intervention for established rhinophyma
Type 4: Ocular Rosacea
Primary features:
- Eye symptoms: redness, dryness, irritation, burning
- May precede skin symptoms
- Eyelid inflammation (blepharitis)
- Sensitivity to light
- Feeling of something in the eye
Often overlooked: Many patients don’t connect eye symptoms to skin condition.
In Indian context:
- Pollution worsens eye symptoms significantly
- Often managed by ophthalmologist without rosacea diagnosis
- Untreated can affect vision
- Should be co-managed with dermatologist and ophthalmologist
Treatment focus: Specific eye drops, lid hygiene, oral antibiotics, coordinated care
Mixed Types (Common)
Most patients have features of multiple subtypes, requiring combination treatment approaches.
What Causes Rosacea: The Science
The Three-Factor Model
1. Genetic predisposition:
- Strong hereditary component
- Specific immune system variants
- Abnormal vascular reactivity
- Skin barrier dysfunction genes
2. Immune dysfunction:
- Overactive innate immune system
- Elevated cathelicidins (antimicrobial peptides)
- Inflammatory cascade activation from triggers
- Microbiome disruption
3. Environmental triggers:
- Activate genetic and immune factors
- Cause acute flushing and chronic inflammation
- Progressive damage accumulates over time
The Demodex Connection
What are Demodex mites?
- Tiny mites naturally living in facial hair follicles
- Everyone has some Demodex
- Rosacea patients have significantly higher numbers
- Particularly Demodex folliculorum and Demodex brevis
How they contribute:
- Trigger immune responses
- Carry bacteria that activate inflammation
- Physical presence irritates follicles
- Explains some treatment responses (ivermectin)
Indian context: Warm climate and humidity may support higher Demodex populations, potentially contributing to rosacea severity.
The Microbiome Factor
Skin microbiome disruption:
- Reduced diversity of beneficial bacteria
- Overgrowth of inflammatory bacteria
- Bacillus oleronius associated with rosacea
- Gut-skin axis increasingly recognized
Implications:
- Explains variable trigger responses
- Supports probiotic research
- Affects antibiotic treatment choices
- Links to gut health management
Rosacea Triggers in India: A Comprehensive Guide
Universal Triggers
Temperature and weather:
- Sun exposure (major trigger, highly relevant in India)
- Cold wind (Delhi winters particularly problematic)
- Hot, humid weather (triggers flushing and inflammation)
- Moving between air conditioning and outdoor heat
- Hot showers or baths
Dietary triggers:
- Spicy foods (ubiquitous in Indian cuisine – a significant challenge)
- Hot beverages (tea, coffee, soups)
- Alcohol (especially red wine, beer)
- Cinnamaldehyde-containing foods (tomatoes, citrus, chocolate)
- Histamine-rich foods (fermented products, some fruits)
Emotional factors:
- Stress (workplace, family, social pressures)
- Anxiety
- Embarrassment (the cruel cycle – rosacea causes embarrassment, embarrassment causes flushing)
- Anger or frustration
Physical factors:
- Exercise (particularly high-intensity in heat)
- Fever or illness
- Hot yoga (very popular in India, very problematic for rosacea)
- Any activity raising core temperature
Skincare and topical products:
- Alcohol-containing products
- Harsh cleansers
- Physical scrubs and exfoliants
- Fragrances (including in toiletries)
- Chemical sunscreens (some formulations)
- High-concentration active ingredients
- Steroid creams (particularly misused in Indian skin)
India-Specific Triggers
Delhi pollution (major factor):
- PM2.5 particles trigger inflammatory responses
- Chemical irritants penetrate compromised barrier
- Oxidative stress activates rosacea pathways
- Year-round concern, peaking in winter
- Creates ongoing “background” inflammation
Delhi’s notorious air quality creates particular challenges for rosacea patients. Our comprehensive guide on surviving Delhi’s heat and pollution discusses anti-pollution strategies relevant for inflammatory conditions.
Delhi winter’s double threat:
- Extreme cold causing immediate vascular reactions
- Moving from freezing outdoor temperatures to heated indoors
- Hot beverages consumed more frequently
- Indoor heating creating dry, irritating air
- Peak pollution coinciding with cold
Our Delhi winter skincare guide addresses environmental challenges that worsen rosacea specifically during winter months.
Indian dietary patterns:
- Spicy curries, chutneys, pickles
- Hot chai and coffee consumption patterns
- Festive eating (heavy, spicy, alcohol-containing foods)
- Street food with chili and spices
- These are cultural staples – complete avoidance is often unrealistic
Ayurvedic and traditional treatments:
- Turmeric in high concentrations (irritating for some)
- Harsh herbal preparations
- Facial steaming (popular home treatment, disastrous for rosacea)
- Hot oil massages on face
- Abhyanga face treatments
Cultural makeup practices:
- Heavy foundation and coverage products
- Occlusive kajal and kohl around eyes
- Wedding and festival makeup (thick, multiple layers, hot conditions)
- Removal with harsh cleansers or wipes
Wedding and festival seasons:
- Multiple stressors combining simultaneously
- Makeup, heat, spicy food, alcohol
- Sleep disruption
- Social and family pressure
- These events reliably trigger severe flares in susceptible patients
Sun exposure patterns:
- Outdoor prayer or religious activities in direct sun
- Farming and outdoor occupations
- Sports and outdoor activities
- Religious festivals outdoors in summer
- UV intensity extremely high in Indian summer
Understanding Steroid Misuse: India’s Rosacea Emergency
The Steroid Problem
This deserves its own section because it’s endemic in India and causes catastrophic rosacea worsening.
What happens:
- Patient develops redness (from rosacea or another condition)
- Visits pharmacy or beautician
- Receives potent steroid cream (betamethasone, clobetasol, mometasone)
- Redness temporarily improves (steroids are anti-inflammatory)
- Stopping cream causes rebound redness – worse than before
- Patient applies more steroid to control rebound
- Cycle of dependency develops
- Skin becomes thin, permanently red, with visible vessels
- Steroid-induced rosacea (rosacea-like dermatitis) develops
Why this is so common in India:
- Prescription steroids are available without prescription in many pharmacies
- Beauticians dispensing prescription medications illegally
- “Fairness creams” containing undisclosed steroids
- Cultural reliance on “pharmacy bhai” recommendations
- Limited awareness of steroid dangers
The devastating outcome:
- Thin, paper-like skin
- Permanent telangiectasias
- Rosacea significantly worsened
- Difficult to treat
- Takes months to years to recover
- May never fully normalize
If you’re using steroid creams on your face: Stop (with medical guidance – sudden stopping can cause severe rebound). See dermatologist immediately.
Our skincare scams guide discusses unsafe products including undisclosed steroids in fairness creams.
Diagnosing Rosacea in Indian Skin
Clinical Diagnosis
Rosacea diagnosis is clinical—based on examination and history, not blood tests or biopsies.
Key diagnostic criteria:
- Persistent central facial redness
- Flushing episodes
- Papules or pustules in central face (without comedones)
- Telangiectasias (visible blood vessels)
- Ocular symptoms
- Positive response to rosacea-specific triggers
Dermatoscopy findings:
- Dilated superficial blood vessels
- Follicular plugging
- Demodex mites may be visible
- Perifollicular scaling
In Indian skin, dermatologists look for:
- Subtle changes in skin tone (dusky vs. bright red)
- Background discoloration in central face
- Vessel patterns invisible to naked eye
- Texture changes indicating subtype
Distinguishing from Similar Conditions
Rosacea vs. Acne:
| Feature | Rosacea | Acne |
|---|---|---|
| Blackheads/whiteheads | Absent | Present |
| Background redness | Present | Usually absent |
| Flushing | Present | Absent |
| Location | Central face | Face, chest, back |
| Onset | Usually 30s-50s | Usually teens-20s |
| Triggers | Heat, spicy food | Hormones, diet |
Rosacea vs. Seborrheic Dermatitis:
- Seborrheic: Yellow, greasy scales; eyebrows, sides of nose, hairline involved
- Rosacea: Red background, central cheeks and nose, flushing, no scales typically
Rosacea vs. Lupus:
- Lupus: Butterfly rash following cheekbones; systemic symptoms; positive blood tests
- Rosacea: Affects nose prominently; no systemic symptoms; triggers cause flushing
Rosacea vs. Perioral Dermatitis:
- Perioral: Specifically around mouth and nose; often steroid-induced
- Rosacea: Central face, may overlap but broader distribution
Rosacea vs. Contact Dermatitis:
- Contact: Related to specific product or exposure; resolves when exposure removed
- Rosacea: Chronic, multiple triggers, persistent background
Our guide on unexpected eczema triggers provides context for distinguishing inflammatory conditions with overlapping presentations.
Medical Treatment: What Actually Works
Topical Treatments
Metronidazole (First-line treatment):
- Anti-inflammatory and anti-Demodex effects
- Available as 0.75% gel or 1% cream
- Once or twice daily application
- Well-tolerated, minimal side effects
- Effective for papulopustular type
- Cost: ₹200-800
- Results: 6-12 weeks for significant improvement
Azelaic Acid (Excellent for Indian skin):
- Anti-inflammatory
- Reduces redness and papules
- Bonus: Treats pigmentation (valuable for Indian patients)
- 15% gel or 20% cream
- Twice daily
- Cost: ₹400-1,200
- Particularly useful for dual concern (rosacea + pigmentation)
Ivermectin 1% Cream (Newer, highly effective):
- Targets Demodex mites directly
- Superior to metronidazole in studies
- Once daily
- Well-tolerated
- Cost: ₹600-1,500
- Best for papulopustular type with high Demodex burden
Brimonidine Gel (For immediate redness reduction):
- Alpha-adrenergic agonist
- Constricts blood vessels
- Reduces redness within 30 minutes
- Lasts 8-12 hours (cosmetic benefit)
- Doesn’t treat underlying inflammation
- Cost: ₹800-2,000
- Useful for special occasions, events
Oxymetazoline Cream (Newer option):
- Similar mechanism to brimonidine
- Reduces persistent erythema
- Once daily
- Recently introduced in India
- Cost: ₹1,000-2,500
Important: All topical treatments need consistent, long-term use. Stopping causes recurrence.
Oral Medications
Doxycycline (Anti-inflammatory dose, first-line for moderate rosacea):
- 40mg modified-release formulation
- Anti-inflammatory (not antibiotic) at this dose
- Reduces risk of antibiotic resistance
- Taken once daily
- Cost: ₹300-800/month
- Timeline: 12-16 weeks for significant improvement
- Side effects: GI upset, photosensitivity
Standard doxycycline (100mg for severe cases):
- Full antibiotic dose
- For severe papulopustular rosacea
- Shorter courses (3-4 months) to prevent resistance
- Cost: ₹200-600/month
- More side effects than low-dose version
Tetracycline (Alternative, more affordable):
- Older but effective
- Twice daily dosing
- Cost: ₹100-300/month
- Side effects: Photosensitivity, GI issues
Azithromycin (For those unable to take tetracyclines):
- Intermittent dosing protocols
- Cost: ₹200-500/course
- Alternative when tetracycline inappropriate
Isotretinoin (Low-dose for resistant cases):
- Very low doses (10-20mg/day or alternate days)
- For severe, treatment-resistant rosacea
- Requires monitoring
- Cost: ₹800-2,500/month
- Not first-line but effective option
Beta-blockers (For flushing):
- Propranolol for severe flushing
- Off-label use
- Reduces frequency and severity of flushing episodes
- Requires cardiac monitoring
- Not suitable for everyone
- Discuss with dermatologist
Professional Procedures
Vascular lasers (Gold standard for Type 1 ETR):
- Pulsed dye laser (PDL)
- KTP laser
- Nd:YAG laser
- Target and destroy visible blood vessels
- Reduce persistent redness
- Multiple sessions needed (3-5)
- Cost: ₹8,000-20,000 per session
- Results: Significant reduction in vessels and redness
Intense Pulsed Light (IPL):
- Non-laser light-based treatment
- Targets blood vessels and pigmentation
- Multiple sessions needed
- Caution for Indian skin: Risk of hyperpigmentation; requires expertise
- Cost: ₹5,000-15,000 per session
Nd:YAG laser (Safer for Indian skin):
- 1064nm wavelength
- Safer for darker skin tones than PDL or IPL
- Treats persistent redness and vessels
- Preferred option for Indian rosacea patients
- Cost: ₹6,000-15,000 per session
Fractional laser (For phymatous changes):
- Addresses skin texture in Type 3
- Stimulates collagen for smoother surface
- Multiple sessions
- Cost: ₹8,000-25,000 per session
Surgical intervention (For rhinophyma):
- Laser resurfacing
- Surgical shaving
- Electrosurgery
- For advanced tissue thickening
- Cost: ₹20,000-80,000
Important: All laser treatments for Indian skin require providers with extensive experience in darker skin types. Our comprehensive guide on chemical peels vs. laser treatments explains how provider expertise affects outcomes.
Ocular Rosacea Treatment
Specific management:
- Lid hygiene (warm compresses, lid scrubs)
- Preservative-free artificial tears
- Topical cyclosporine eye drops
- Oral doxycycline (helps ocular rosacea)
- Ophthalmology co-management essential
- Avoid makeup near eyes during flares
Building Your Rosacea Skincare Routine
The Core Principle: Less Is More
Rosacea skin is reactive skin. Every unnecessary product is a potential trigger. Unlike complex routines recommended for other conditions, rosacea management requires radical simplification.
Golden rules:
- Fewer products = fewer potential triggers
- Everything on your skin must earn its place
- Introduce one new product at a time
- Wait 2-4 weeks before adding another
- When in doubt, leave it out
Cleanser Selection (Critical)
What to look for:
- Extremely gentle, non-foaming or light-foaming
- Fragrance-free
- No alcohol
- pH balanced (around 5.5)
- No scrubbing particles
- Rinse-off cleansers preferred over wipes
What to avoid absolutely:
- Sulfates (SLS, SLES)
- Fragrances or essential oils
- Alcohol-based toners or cleansers
- Scrubs or exfoliating cleansers
- Hot water (always lukewarm)
Application technique:
- Fingertips only (no washcloths)
- Gentle circular motions
- Lukewarm or cool water
- Pat dry with soft cloth (don’t rub)
- Be especially gentle around nose and cheeks
Affordable options:
- Cetaphil gentle skin cleanser (₹400-800)
- La Roche-Posay Toleriane hydrating cleanser (₹1,200-2,000)
- CeraVe hydrating cleanser (₹800-1,500)
- Bioderma Sensibio foaming gel (₹1,000-1,800)
Moisturizer (Essential Barrier Support)
Why crucial for rosacea:
- Strengthens compromised barrier
- Reduces sensitivity and reactivity
- Calms inflammation
- Reduces transepidermal water loss
Key ingredients:
- Ceramides (barrier restoration)
- Niacinamide (anti-inflammatory, supports barrier)
- Centella asiatica (calming, anti-inflammatory)
- Hyaluronic acid (hydration)
- Panthenol/B5 (soothing)
- Green tea extract (antioxidant)
Avoid:
- Fragrance
- Essential oils
- High concentrations of acids
- Retinol (initially)
- Vitamin C (test carefully—can irritate some)
Affordable options:
- CeraVe moisturizing cream (₹800-1,500)
- La Roche-Posay Toleriane sensitive (₹1,200-2,200)
- Minimalist 2% Niacinamide + 0.3% Zinc (₹500-700)
- Cetaphil moisturizing lotion (₹400-800)
Sunscreen (Non-Negotiable)
Why rosacea patients must use sunscreen:
- UV is a major universal trigger
- Delhi sun intensity extremely high
- Reduces flushing episodes
- Prevents pigmentation changes
Best formulations for rosacea:
- Physical/mineral sunscreens (zinc oxide, titanium dioxide)
- Gentler than chemical sunscreens
- Less likely to trigger rosacea
- Provides additional anti-inflammatory benefits from zinc
Texture considerations:
- Lightweight, non-comedogenic
- Soothing formulations
- Tinted options may help camouflage redness
Avoid:
- Chemical filters (benzophenone, PABA—common triggers)
- Fragranced sunscreens
- Alcohol-heavy formulations
Recommended options:
- La Roche-Posay Anthelios mineral SPF 50 (₹1,800-2,500)
- CeraVe Mineral Sunscreen SPF 30 (₹1,200-1,800)
- Minimalist SPF 50 PA++++ (₹500-800)
- EltaMD UV Elements (₹3,000-4,500)
Application: Liberal amount, reapply every 2-3 hours outdoors
Complete Morning Routine
- Gentle cleanser (lukewarm water, fingertips)
- Medical treatment (metronidazole, azelaic acid, or ivermectin as prescribed)
- Moisturizer (wait for treatment to absorb)
- Mineral sunscreen (non-negotiable)
- Optional: Brimonidine for special occasions when minimal redness desired
Total time: 5-7 minutes
Complete Evening Routine
- Gentle cleanser (double cleanse if wearing makeup or sunscreen)
- Medical treatment (if twice daily) or different prescription as directed
- Soothing serum (centella, niacinamide, or panthenol if tolerated)
- Moisturizer (slightly richer at night)
Total time: 7-10 minutes
What to Remove From Routine
Eliminate immediately:
- Toners with alcohol or fragrance
- Physical exfoliants (scrubs, brushes, dermaplaning)
- High-concentration AHAs/BHAs initially
- Retinoids (until rosacea controlled, then introduce very carefully)
- Essential oil-containing products
- Multiple different products
Potentially reintroduce carefully later:
- Low-concentration azelaic acid (often beneficial)
- Niacinamide (generally well-tolerated)
- Very low retinaldehyde (after rosacea stabilized)
- Gentle chemical exfoliation (once monthly maximum)
Managing Triggers: Practical Strategies for Indian Life
The Food Challenge
The reality: Complete elimination of spicy food is culturally unrealistic for most Indian patients.
Practical approach:
- Identify YOUR specific triggers (not everyone reacts the same)
- Keep food diary for 4-6 weeks
- Identify worst offenders and eliminate or reduce those
- Gradual reduction rather than complete elimination
- Cool foods and room-temperature beverages when possible
- Sip cool water alongside hot foods to reduce flushing
Specific Indian food strategies:
- Request “mild spice” at restaurants
- Add cooling elements (raita, cucumber) to spicy dishes
- Reduce chili gradually in home cooking
- Choose cooler preparations when available
- Identify which spices specifically trigger (capsaicin in chili vs. other spices)
Cooling replacements:
- Lassi instead of hot chai when possible
- Cooled herbal teas
- Coconut water
- Cool cucumber or mint-infused water
Sun and Heat Management
Delhi-specific strategies:
- Plan outdoor activities before 10 AM or after 5 PM
- Carry a physical sun umbrella (genuinely effective)
- Broad-brimmed hat
- Cooling face mist with thermal spring water
- Car AC before stepping out to reduce temperature shock
Exercise modifications:
- Choose indoor, air-conditioned exercise when possible
- Cool environment always preferred
- Cool shower immediately after exercise
- Apply cool compress to face post-workout
- Carry cooling spray during exercise
Yoga modifications:
- Avoid hot yoga completely
- Choose room-temperature yoga
- Restorative or yin yoga preferred
- Pranayama (breathing exercises) beneficial for stress reduction without heat
Stress Management in Indian Context
Cultural stressors:
- Wedding planning
- Family obligations and expectations
- Work pressure in competitive urban environments
- Festive season demands
- Traffic and commuting stress (Delhi-specific)
Practical stress reduction:
- Regular meditation (Headspace, Calm, or simple breathing exercises)
- Consistent sleep schedule (7-9 hours)
- Physical exercise (cool environment, appropriate intensity)
- Professional counseling when stress becomes chronic
- Saying “no” when necessary
- Delegate during high-stress periods
During unavoidable high-stress events:
- Pre-treat with prescribed medications
- Prepare soothing skincare products for immediate post-event care
- Have cooling mist and gentle cleanser accessible
- Realistic expectation that some flaring may occur
Festive Season Survival Guide
Wedding and festival preparation:
- Start medical treatment 4-6 weeks before (not during)
- Choose experienced makeup artist familiar with rosacea
- Test all makeup products 2-4 weeks before event
- Brief artist on your condition and sensitivities
- Request mineral-based, fragrance-free products
- Carry gentle cleansing option for quick removal
Makeup that works with rosacea:
- Mineral foundation
- Green-tinted color-correcting primer (counteracts redness)
- Physical SPF under foundation
- Fragrance-free everything
- Avoid heavy coverage requiring harsh removal
Post-event care:
- Remove makeup immediately after event
- Gentle double cleanse
- Apply prescribed treatment
- Soothing moisturizer
- Keep face cool during event if possible
Pollution Protection
Daily anti-pollution strategy:
- Double cleanse every evening (non-negotiable)
- Physical sunscreen provides partial barrier
- Antioxidant protection (check tolerance first)
- Indoor air purifier
- Minimize outdoor exposure during peak pollution (AQI>200)
- Check AQI before outdoor activities
Special Considerations for Indian Women with Rosacea
Hormonal Connections
Why rosacea often worsens with:
- Menopause (hot flashes trigger flushing)
- Menstrual cycle changes
- Hormonal contraceptives (some affect rosacea)
- Pregnancy (mixed effects—some improve, some worsen)
Management:
- Track hormonal patterns and flushing
- Discuss hormonal influences with dermatologist
- Consider hormonal evaluation if significant correlation
- Some medications may need adjustment
Pregnancy and Breastfeeding
Safe topical options:
- Azelaic acid (generally considered safe)
- Gentle moisturizers and mineral sunscreen
- Physical cooling measures
Avoid during pregnancy:
- Oral antibiotics in first trimester (discuss with obstetrician and dermatologist)
- Isotretinoin (absolutely contraindicated)
- Some laser treatments
After delivery:
- Rosacea may flare postpartum
- Many medications safe during breastfeeding
- Consult dermatologist for appropriate postpartum management
Makeup and Confidence
The emotional reality: Rosacea significantly impacts confidence. Many Indian women feel unable to leave home without heavy makeup coverage.
Better approach:
- Color-correcting primer reduces amount of foundation needed
- Building toward comfortable minimal coverage
- Treatment reduces background redness, requiring less concealment
- Accepting skin condition doesn’t define worth
Rosacea and Related Health Conditions
Cardiovascular Connection
Research suggests:
- Rosacea patients have higher rates of cardiovascular disease
- Shared inflammatory mechanisms
- Increased monitoring recommended for heart health
- Discuss with physician for comprehensive care
Gut Health Connection
Growing evidence:
- Increased rates of irritable bowel syndrome in rosacea patients
- Small intestinal bacterial overgrowth (SIBO) association
- Gut microbiome influence on skin inflammation
- Probiotic research promising
Practical implications:
- Gut health management may complement skin treatment
- Probiotic supplementation worth discussing with doctor
- Anti-inflammatory diet supports both gut and skin
- H. pylori treatment improves rosacea in some patients
Neurological Connections
Interesting associations:
- Increased Parkinson’s disease risk (shared inflammatory mechanisms)
- Migraine association
- Both involve vascular reactivity
- Not cause and effect, but shared pathways
Psychological Impact
Common psychological effects:
- Social anxiety (avoiding situations where flushing might occur)
- Depression
- Reduced self-esteem
- Professional concerns about appearance
- Relationship impact
Indian-specific concerns:
- Marriage prospects in communities valuing appearance
- Professional image in client-facing roles
- Social pressure at gatherings, functions, festivals
Addressing psychological impact:
- Acknowledge emotional burden as valid
- Discuss openly with dermatologist
- Professional counseling if significantly impacting life
- Support communities online and in-person
- Remember: Rosacea is treatable; don’t suffer in silence
Our guide on what to expect at your first dermatology appointment includes discussing emotional impacts with your doctor.
Long-term Management: Living with Rosacea
Setting Realistic Expectations
What treatment achieves:
- Significant reduction in redness and inflammation
- Fewer and less severe flares
- Prevention of progression
- Improved quality of life
- Better skin texture
What treatment doesn’t achieve:
- Complete cure
- Prevention of all flares
- Instant results
- Permanent elimination without maintenance
Timeline:
- 4-6 weeks: Initial improvement possible
- 12 weeks: Significant improvement with consistent treatment
- 6 months: Optimal baseline achieved
- Ongoing: Maintenance therapy required
Maintenance Phase
Long-term strategy:
- Continue topical treatments even when skin looks good
- Regular dermatologist monitoring (every 3-6 months)
- Seasonal adjustments (winter vs. summer protocols)
- Medication modifications as needed
- Ongoing trigger management
What to monitor:
- Frequency and severity of flushing episodes
- New lesions or vessel formation
- Eye symptoms
- Changes in nose or skin texture
- Response to new products or treatments
Building Your Rosacea Management Plan
The comprehensive approach:
- Medical treatment: Topical and/or oral medications as prescribed
- Trigger identification and avoidance: Personalized trigger diary
- Optimized skincare: Minimal, gentle, soothing products
- Environmental protection: Sun, pollution, temperature management
- Lifestyle modifications: Diet, stress, exercise adaptations
- Professional treatments: Laser when appropriate
- Psychological support: Address emotional impact
- Regular monitoring: Consistent dermatology follow-up
Common Mistakes to Avoid
Mistake #1: Using Steroid Creams
Already discussed extensively—most damaging mistake with potentially permanent consequences.
Mistake #2: Aggressive Exfoliation
The problem: Scrubs, acids, dermaplaning worsen rosacea.
The solution: Eliminate all exfoliation initially. Reintroduce only under dermatologist guidance.
Mistake #3: Facial Steaming
The problem: Popular in Indian home remedies; heat triggers rosacea.
The solution: Never steam face with rosacea.
Mistake #4: Multiple New Products Simultaneously
The problem: Can’t identify which product triggers reaction.
The solution: One new product at a time, 2-4 week intervals.
Mistake #5: Stopping Treatment When Skin Improves
The problem: Rosacea is chronic; improvement requires maintenance.
The solution: Continue treatment at maintenance level indefinitely.
Mistake #6: Treating as Acne
The problem: Acne treatments (benzoyl peroxide, salicylic acid) worsen rosacea.
The solution: Accurate diagnosis before any treatment.
Mistake #7: Visiting Beautician for Treatment
The problem: Facials, extractions, peels all worsen rosacea.
The solution: Dermatologist-only management for all rosacea treatments.
Our guide on dermatologist vs. beautician is particularly relevant for rosacea patients who often seek salon treatments first.
When to See a Dermatologist
If You Suspect Rosacea
Consultation indicated if:
- Persistent central facial redness
- Flushing episodes without clear cause
- Acne-like bumps not responding to acne treatments
- Visible blood vessels on cheeks or nose
- Burning or stinging sensations
- Eye redness and irritation accompanying skin symptoms
- Progressive thickening of nose
Don’t wait: Rosacea progresses without treatment. Early intervention prevents rhinophyma and permanent vessel damage.
Urgency Levels
Immediate (within days):
- Severe sudden worsening
- Eye pain or vision changes
- Suspicion of steroid-damaged skin requiring supervised withdrawal
Soon (within weeks):
- New onset of symptoms
- Significant psychological impact
- Spreading involvement
Routine (within months):
- Mild symptoms for initial evaluation
- Annual monitoring check-ups
Our comprehensive guide on booking your first dermatology appointment helps prepare for your consultation.
Cost of Managing Rosacea in India
Realistic Budget Expectations
Basic management (₹2,000-4,000/month):
- Topical metronidazole or azelaic acid
- Gentle cleanser
- Moisturizer
- Mineral sunscreen
- Initial consultation
Moderate management (₹5,000-10,000/month):
- Premium topical treatments
- Quality skincare products
- Oral medication if needed
- Regular dermatology visits
- Quarterly professional consultations
Comprehensive management (₹15,000+/month):
- Medical treatments
- Quality products
- Professional procedures (laser)
- Regular monitoring
- For those wanting optimal results
Government hospital options:
- Significantly subsidized consultations
- Generic medications much cheaper
- May have waiting times
- Good for budget-conscious patients
Conclusion: Your Face Doesn’t Have to Be Always Red
Rosacea in Indian skin is under-diagnosed, frequently mismanaged, and unnecessarily suffered through. The persistent redness, flushing episodes, burning sensations, and progressive changes you’ve been dismissing as “sensitive skin” or “my complexion” may be a treatable medical condition.
The key takeaways:
Rosacea looks different in Indian skin—more dusky and uneven than bright red, making recognition challenging. It’s frequently confused with acne, eczema, or simple pigmentation. Steroid creams, a common first response in India, catastrophically worsen rosacea. India’s climate, diet, and environmental factors create unique challenges requiring specific management strategies. Treatment is highly effective—most patients achieve significant improvement with appropriate medical care.
Your action plan:
- Stop all steroid creams immediately (with medical supervision)
- Simplify skincare to gentle, fragrance-free essentials
- Begin trigger identification diary
- Make dermatology appointment for accurate diagnosis
- Follow prescribed treatment consistently
- Protect from sun and pollution daily
- Be patient—consistent treatment delivers results
You deserve a face that isn’t always red, burning, or reactive. With accurate diagnosis and appropriate treatment, most rosacea patients achieve excellent control and dramatically improved quality of life.
Your skin can be calm, comfortable, and confident. That journey starts with recognizing what you might actually be dealing with—and seeking the right help.
Dr. Shruti Patil is a board-certified dermatologist at Dr. Mahajan Skin To Bone Clinic, Pashim Vihar, New Delhi. With extensive experience diagnosing and treating rosacea in Indian skin, she specializes in managing this challenging condition within the context of India’s unique climate, dietary culture, and environmental factors.
Experiencing persistent facial redness, flushing, or burning that isn’t responding to treatments? Schedule a consultation for accurate diagnosis and a personalized rosacea management plan tailored to your specific skin type, triggers, and lifestyle.
Leave a Reply